

Dr. Dr. Susanne Kluba
Specialist for oral and maxillofacial surgery
Content
Dear colleagues, dear people responsible for baby health,
Cranial deformations in infancy have been a frequently observed phenomenon for almost three decades. The vast majority of them are positional and only rarely, premature cranial suture occlusions, so called craniosynostoses, are causative. Despite a great deal of scientific work on the subject, positional deformations are still the subject of very controversial discussions, even among experts. Attitudes to the relevance and need for therapy of this phenomenon vary greatly and in different therapist groups, especially in the evaluation of helmet therapy. At the same time, however, parents and caregivers have a great need for information and advice, and controversial statements can lead to uncertainty on the parent side. In the interest of the affected families, the parents’ concerns should be taken seriously and addressed, and consulting or, if necessary, referral to a craniofacial specialist should take place.
As a health professional, midwife, or paediatrician, you have the opportunity to recognise head deformations at an early stage and initiate a reasonable therapy. Early parental education and recommendations for active prophylaxis are even more important. We would like to support parents or doctors
- in correctly assessing the shape of the head and
- educate parents about positional head deformations at an early stage and provide them with simple preventive measures.
What we have summarised here is basic information on the development, diagnosis and therapy of positional head deformations as well as our preventive approach. You can also download these, including all source references, as a document here and are welcome to pass them on. We are always available for professional exchange and are looking forward to your feedback on the preventive baby head protection, which can be sent to you at a small nominal fee.
Yours sincerely,

Causes of head deformations
One of the multifactorial, not causally proven, influencing factors for the increasingly observed cranial positional deformations these days is assumed to be the recommendation for supine positioning as prevention of Sudden Infant Death Syndrome (SIDS), which was put out in 1992. This recommendation led to a significant reduction in SIDS deaths. However, an increase in the incidence of skull deformations was subsequently observed. Among others, Argenta et al. report an increase in occipital flattening of up to 600 %. Depending on the inclusion criteria, an incidence of up to 46.6 % for positional cranial deformations is reported in the literature, up to over 80 % on the day of discharge of preterm infants.
In addition to this relevant postnatal risk factor, a number of other risk factors are known for the development of positional skull deformations. These include, among others:
Prenatal factors:
- Male gender
- Primipara
- Intrauterine predicaments
Postnatal factors:
- Supine position
- Restricted head movement (torticollis)
- Side preference
- Bottle feeding without changing position
- Low “tummy time”
- Developmental delay, low activity
Postnatal factors:
- Forceps or suction delivery
- High birth weight
- Prematurity
- Large head circumference

Development and clinical picture
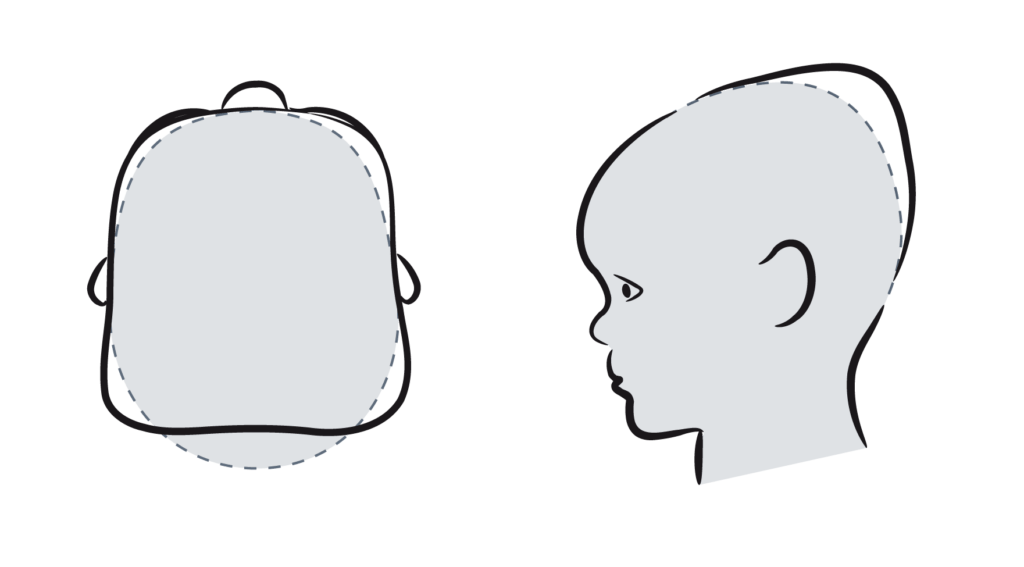
The cranial sutures are physiologically not yet ossified at birth. However, this means that the skull is still easily deformable by external forces, especially within the first months of life.
Positional deformations may clinically show as plagiocephaly with unilateral occipital flattening as the main feature or brachycephaly with bilateral occipital flattening. Mixed forms are common. Furthermore, a shift of the ear axis and facial asymmetries can occur. Argenta has incorporated the relevant criteria into its clinical classification.
.
Verlaufsformen der Plagiozephalie (Schiefschädel)

SLIGHT LATERAL FLATTENING
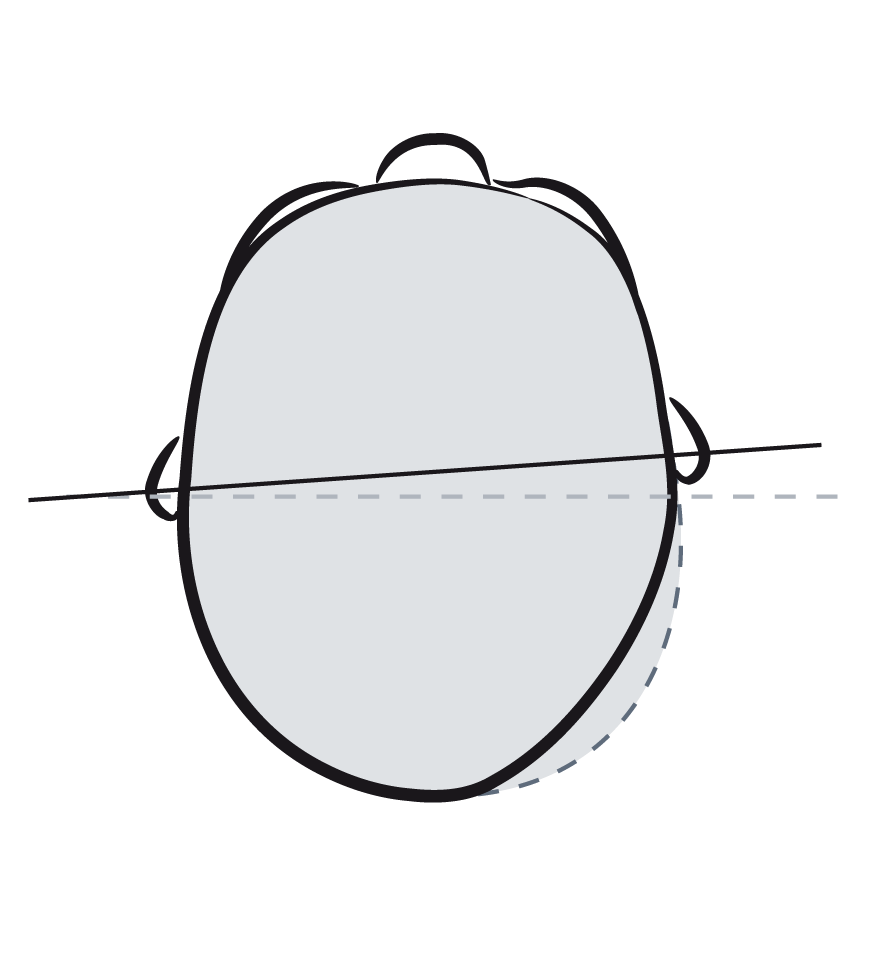
MIDDLE LATERAL FLATTENING WITH DISPLACEMENT OF THE EAR
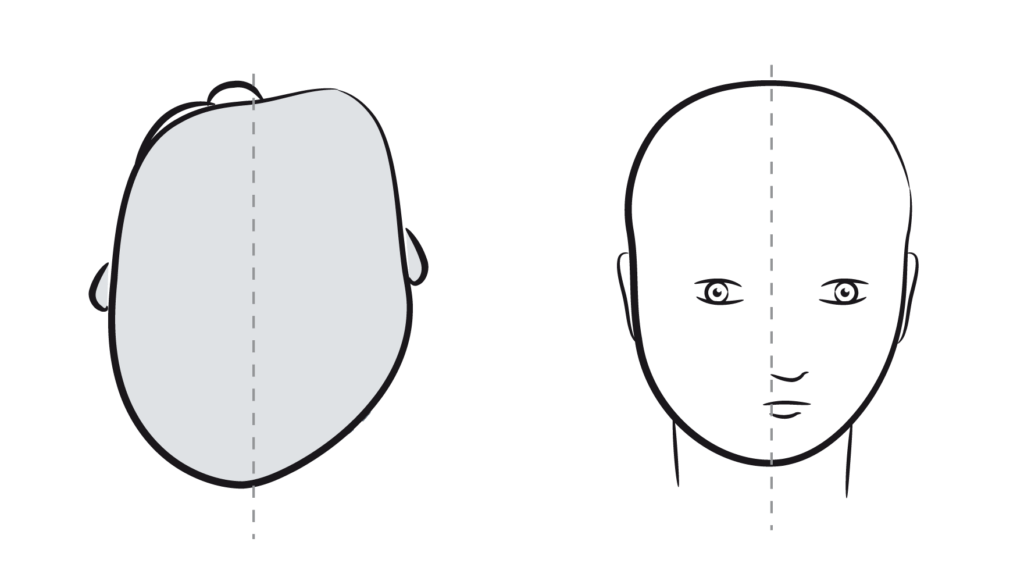
STRONG LATERAL FLATTENING WITH SHIFTING OF THE FACE
PROGRESSIONS OF BRACHYCEPHALY (SHORT SKULL)
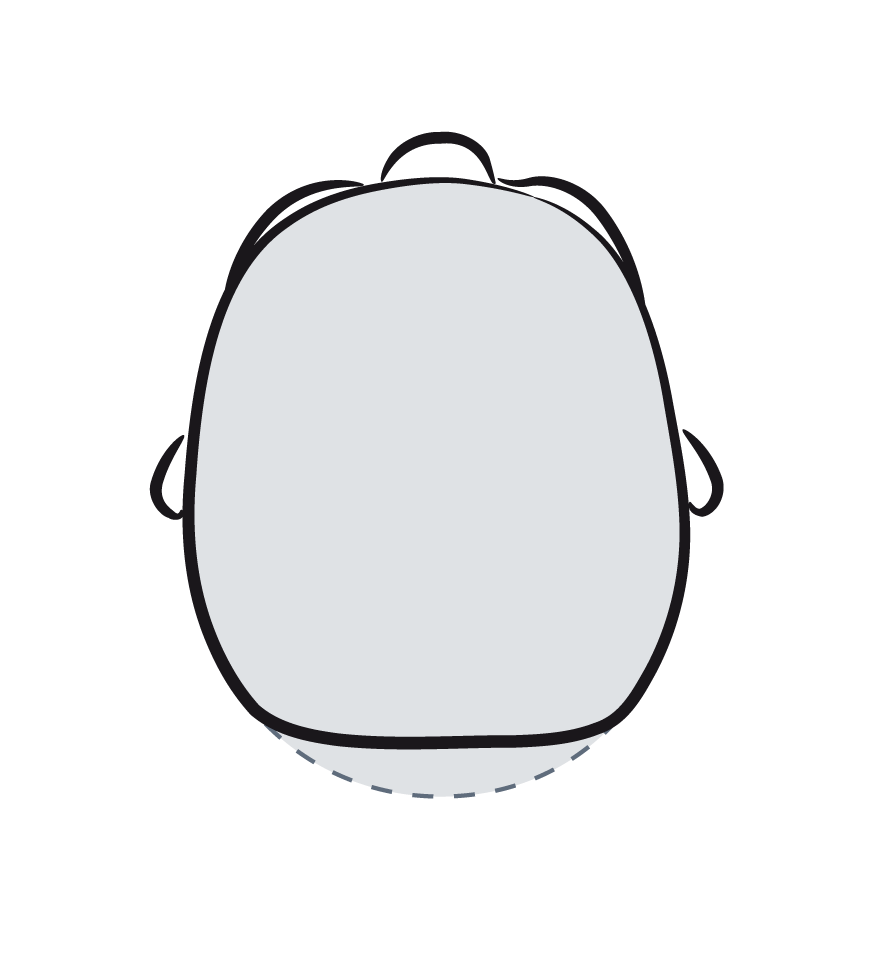
SLIGHT FLATTENING OF THE BACK OF THE HEAD
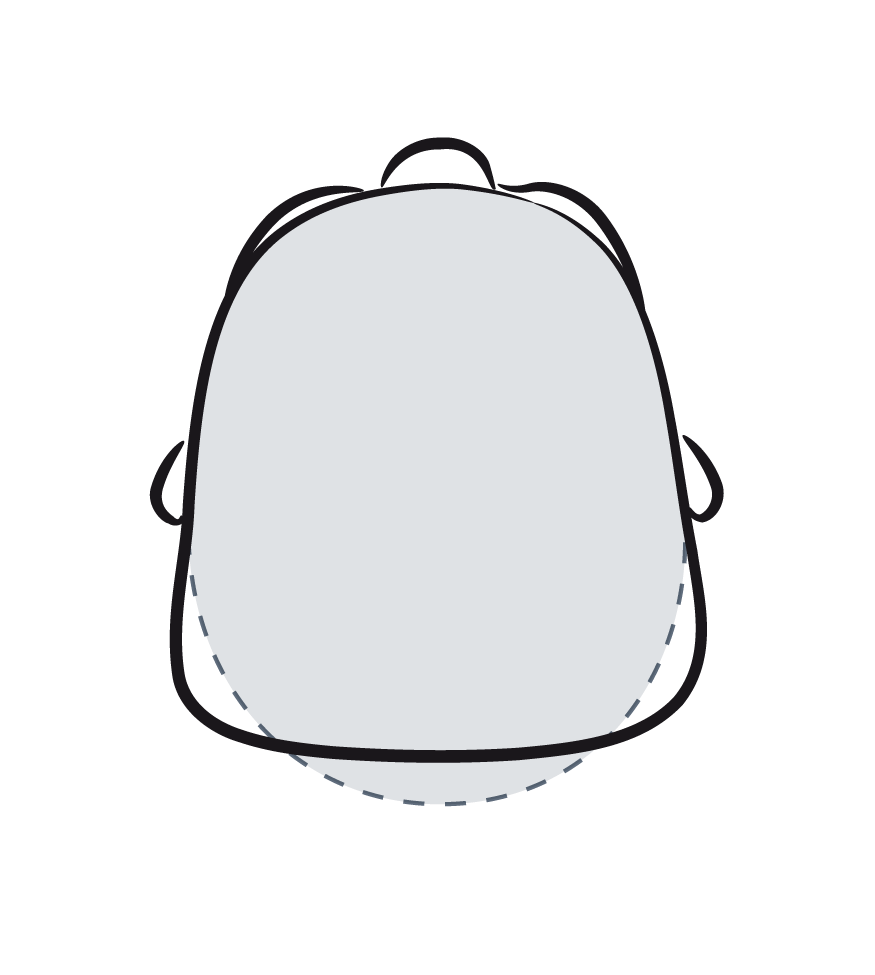
MEDIUM FLATTENING OF THE BACK OF THE HEAD
STRONG FLATTENING WITH RAISED BACK OF THE HEAD
Diagnosis of positional head deformation
Anamnesis and clinical picture are decisive for the diagnosis. A careful collection of the medical history, especially with regard to risk factors and course, in combination with the typical clinical picture, often allow the diagnosis to be narrowed down. In differentiating positional head deformations from cranial suture occlusions, the progression is decisive, in addition to the typical appearance. While positional deformations show an improvement tendency, in craniosynostoses, the deformation becomes more pronounced over time and does not show any spontaneous improvement. A radiation-free surface scanning method, such as 3D stereophotogrammetry, can be used for diagnostics and progress monitoring. To exclude a premature cranial suture closure, cranial sonography is suitable as a non-invasive and radiation-free procedure.
If the deformations are already evident at an earlier age or if the deformation is conspicuous beyond the age of 4 months, an introduction to a craniofacial centre or a helmet consultation should be considered. This introduction should and can be made promptly and in parallel with other therapeutic approaches such as physiotherapy or osteopathy, as the success of therapy with indicated or desired helmet therapy also depends on the age in the beginning of therapy.
Informationsmaterial Bestellen

Therapieempfehlung bei lagebedingten Kopfverformungen
Depending on the severity, conspicuousness, requests of the parents and the accompanying circumstances, various therapeutic approaches are available. In mild cases, a spontaneous improvement can be waited for and supported with simple positioning measures. In general, active and passive positioning therapy, applied as early and consistently as possible, is an important preventive as well as therapeutic approach. This includes actively repositioning the child or using positioning aids. In studies, positioning pillows to support pressure-relieving positioning are described as comparably effective or even superior to physiotherapy. However, most of these products do not comply with the prevention recommendations to reduce the risk of SIDS by not using pillows in the cot.
Another important therapeutic approach oriented towards possible causes is the best possible promotion of mobility and elimination of possible movement limitations (torticollis). Here, physiotherapy is an important part of therapy. As a maximum variant of therapy, helmet therapy is available for severe cases as a non-invasive treatment with few side effects. Helmet therapy has been described as effective in many studies. However, it requires good cooperation from parents and is time sensitive. Starting therapy before 6 months of age, ideally between 5 and 6 months of age, shows a statistically better outcome than therapy started later. Generally, all measures can also be combined and applied in parallel, depending on the case, and thus also lead to an improvement of the therapy effect.

Fokus auf Prävention lagebedingter Kopfverformungen
Especially in view of the very controversial helmet therapy, which is associated with high self-payed costs of about 1000-2000 EUR, we consider prevention and education to be the most promising approach. The aim is to reduce the severity of the manifestation and thus avoid or reduce the need for costly therapies. All preventive measures have a greater protective influence the sooner they take place – from the first day of life, since within the first months of life, the skull has both the greatest growth potential and the greatest susceptibility to positional deformations. Due to the increased resting on a still mildly flattened skull bone, this deformation can worsen itself, so tertiary prevention is indicated here as well.
ORDER INFORMATION MATERIAL
General prevention measures
The most obvious, cheapest and most effective measure is to inform and instruct the parents, e.g. in the context of one of the first preventive medical check-ups at the paediatrician’s or during the midwife aftercare. The pathogenesis as well as possible preventive measures to avoid one-sided positioning should be addressed. These are:
- Carrying babies in slings or baby carriers,
- Breastfeeding or bottle feeding in alternate drinking positions
- Placing the cot with different orientation to the window
- Approaching the infant from different sides,
- and, under observation, the promotion of motor development in the prone position (“tummy time”) during the infants’ waking hours.
Prevention through pressure-relieving positioning
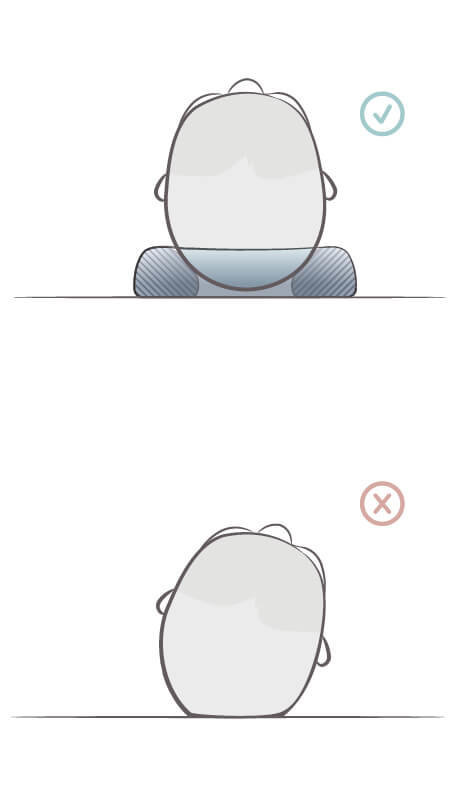
Furthermore, the German Society for Surgery, together with the German Society for Paediatric Surgery, among others, recommends special positioning pillows as a preventive measure, which allow the back of the head to freely float. This is a simple and cost-effective preventive measure. Its effectiveness has been proven by studies.
However, recommendations for the prevention of SIDS include, among other things, the recommendation to lie on the back and not to use large-volume pillows. Our small-volume and growing Medibino positioning ring with free floating of the back of the head and support of the supine position, which is protective for SIDS – but still allows free movement of the head – complies with these two recommendations for preventative measures.
Due to its small, flexible shape, it can be used not only in the cot but also in prams and infant carriers, thus further minimising the physically demanding lying time. The Medibino® has been certified as a medical device with corresponding biocompatibility and risk management testing for the prevention of positional deformations.
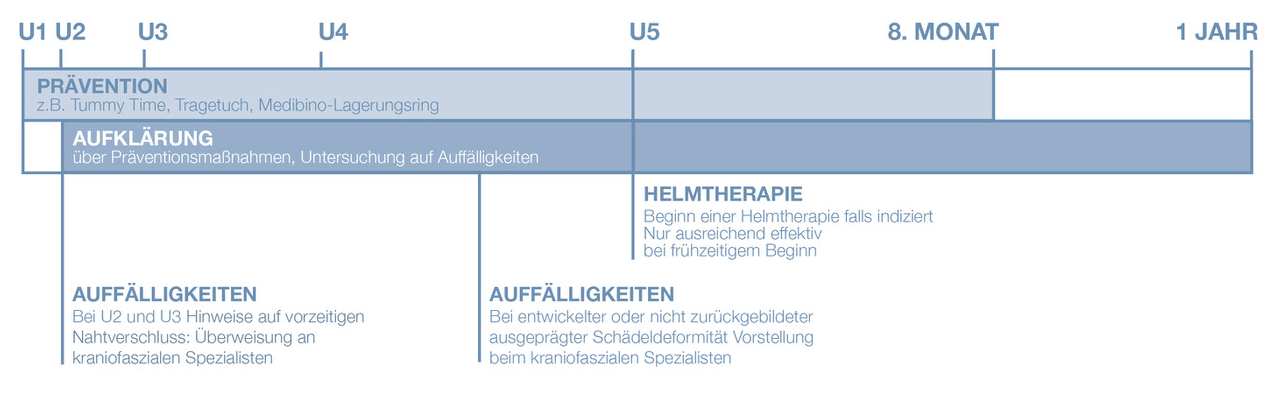
RECOMMENDATIONS FOR PAEDIATRICIANS
As part of the preventive medical check-ups U2, U3 and U4 >
Screening for cranial deformations, educating and instructing parents on the recommended preventive measures to reduce the risk of SIDS and positional cranial deformations.
In case of limited mobility, torticollis etc. >
Additional physiotherapy and/or manual therapies in case of conspicuous or persistent deformation
4th month of life or at parents’ request >
Referral to a craniofacial specialist, craniofacial centre or helmet consultation for quantification of severity, further diagnosis and therapeutic recommendation.
Referral should definitely be proposed early and generously due to decreasing plasticity and should be made promptly.
Please feel free to contact us if you have any further questions or comments: info@kluba-medical.com
For a personal talk, please call us on +49 (0) 211 5421 2590
We will be happy to provide you with information material for you and your patients on the topic of preventing, recognising and treating positional head deformations for your practice. Feel free to contact us or send us an email with the subject “Info package head deformation” to info@kluba-medical.com
ORDER INFORMATION MATERIALBibliography
American Academy of Pediatrics Task Force on Infant Positioning and SIDS.
Positioning and sudden infant death syndrome (SIDS): update. Pedia-trics. 1996;98:1216.
Argenta LC, David LR, Wilson JA, Bell WO.
An increase in infant cranial deformity with supine sleeping position. J Craniofac Surg. 1996;7(1):5-11.
Mawji A, Vollman AR, Hatfield J, McNeil DA, Sauvé R.
The incidence of positional plagiocephaly: a cohort study. Pediatrics. 2013;132(2):298-304.
Yang W, Chen J, Shen W.
et al. Prevalence of positional skull deformities in 530 premature infants with a corrected age of up to months: a multicenter study. BMC Pediatr. 2019;19(1):520. 5
Willis S, Hsiao R, Holland RA, Lee K,Pitetti K:
Measuring for nonsynostotic head deformities in preterm infants during NICU management: A pilot study. Early Hum Dev. 2019;131:56-62. 6 Steinberg JP, Taub PJ : Increase in positional head shape deformities prompt look at risk factors, treatments. AAP News Dec 2014;35(12) 8.
Renz-Polster H, De Bock F.
Deformational plagiocephaly: The case for an evolutionary mismatch. Evol Med Public Health. 2018; 2018(1):180–185.
Littlefield TR, Kelly KM, Reiff JL, Pomatto JK.
Infant car seats, carriers,bouncy seats and swings: their role in deforma-tional plagiocephaly.J Prosthet Orthotot. 2003;15(3):102–106.
Linz C, Kunz F, Böhm H, Schweitzer T:
Positional skull deformities—etiology, prevention, diagnosis, and treat-ment. Dtsch Arztebl Int. 2017;114: 535-42.
Argenta L, David L, Thompson J:
Clinical classification of positional plagiocephaly. J Craniofac Surg. 2004;15(3):368–372. 11 Loveday BP, de Chalain TB: Active counterposi-tioning or orthotic device to treat posi-tional plagiocephaly? J Craniofac Surg. 2001;12(4):308–31.
Loveday BP, de Chalain TB:
Active counterpositioning or orthotic device to treat posi-tional plagioce-phaly? J Craniofac Surg. 2001;12(4):308–31.
Hutchison BL, Hutchison LAD, Thompson JMD, Mitchell EA: Plagiocephaly and brachycephaly in the first two years of life: a prospec-tive cohort study. Pediatrics. 2004;114:970–80.
Bialocerkowski AE, Vladusic SL, Wei NC.
Prevalence, risk factors, and natural history of positional plagiocephaly: a systematic review. Dev Med Child Neurol. 2008;50:577-86.
Collet BR, Breiger DA, King DA, Cunningham MI, Speltz MA. Neurodevelopmental Implications of Deformational Plagiocephaly. J Dev Behav Pediatr. 2005;26(5):379-389.
Miller RI, Clarren SK: Long-term developmental outcomes in pa-tients with deformatio-nal plagiocephaly.
Pediatrics. 2000;105(2):e26 .
Collett BR, Gray KE, Starr JR, Heike CL, Cunningham ML, Speltz ML. Development at age 36 months in children with deformational pla-giocephaly. Pediatrics. 2013;131:e109.
Kordestani RK, Patel S, Bard DE, Gurwitch R, Panchal J. #Neu-rodevelopmental developmental delays in children with deformational plagiocephaly. Plast Reconstr Surg. 2006;117(1):207-18; discussion 219-20.
Siatkowski RM, Fortney AC, Nazir SA, Cannon SL, Panchal J, Francel P, Feuer W, Ahmad W. Visual field defects in deformational posterior plagiocephaly. J AAPOS. 2005;9(3):274-8.
Balan P, Kushnerenko E, Sahlin P, Huotilainen M, Näätänen R, Hukki J. Auditory ERPs reveal brain dysfunction in infants with pla-giocephaly.
J Craniofac Surg. 2002;13(4):520-526.
St John D, Mulliken JB, Kaban LB, Padwa BL.
Anthropometric analysis of mandibular asymmetry in infants with defor-mational posterior plagiocephaly. J Oral Maxillofac Surg. 2002;60:873-877.
Kluba S et al.:
Malocclusion in the primary dentition in children with and without de-for-mational plagiocephaly. Clin Oral Investig. 2016;20(9):2395–2401.
Wilbrand JF, Seidl M, Wilbrand M, et al.:
A prospective randomized trial on preventative methods for posi-tional head deformity: physiotherapy versus a positioning pillow. J Pediatr. 2013;162(6):1216–1221.
Van Vlimmeren LA et al.:
Torticollis and plagiocephaly in infancy: therapeutic strate-gies. Pediatr Rehabil. 2006;9(1):40–46.
Kaplan S, Coulter C, Sargent B.
Physical therapy management of congenital muscular torticollis: a 2018 evidence-based clinical practice guideline from the APTA Academy of Pediatric Physical Therapy. Pediatr Phys Ther. 2018;30(4):240-290.
Kluba S, Kraut W, Calgeer B, Reinert S, Krimmel M.
Treatment of positional plagiocephaly-helmet or no helmet?. J Cranio-maxillofac Surg. 2014;42(5):683–688. 26 Naidoo SD, Skolnick GB, Patel KB, Woo AS, Cheng AL.
Long-term outcomes in treatment of deformational plagiocephaly and brachycephaly using helmet therapy and repositioning: a longitudinal co-hort study. Childs Nerv Syst. 2015;31(9):1547-1552.
Kluba S, Kraut W, Reinert S, Krimmel M.
What is the optimal time to start helmet therapy in positional plagioce-phaly?. Plast Reconstr Surg. 2011;128(2):492–498.
Flannery AM, Tamber MS, Mazzola C, et al.:
Congress of neurological surgeons systematic review and evidence-ba-sed guidelines for the management of patients with positional plagioce-phaly: ex ecutive summary. Neurosurgery. 2016;79:623–24.
Persing J. Prevention and management of positional skull defor-mities in infants.
Am Acad Pediatr. 2017;112:199–202.
Aarnivala H et al.:
Preventing deformational plagiocephaly through parent guidance: aran-domized, controlled trial. Eur J Pediatr. 2015;174(9):1197–1208.
Deutsche Gesellschaft für Chirurgie (19. März 2014).
Chirurgen empfehlen spezielle Kissen für Neugeborene, Schlafen in Rü-ckenlage verformt häufig das Babyköpfchen. Pressemitteilung 131. Kon-gress der Deutschen Gesellschaft für Chirurgie. Abgerufen 26.07.2020 von https://www.dgch.de/fileadmin/media/presse/DGCH_Pressemap-pe_Vorab-PK.pdf.
Ohman A. A Specially Designed Pillow Can Decrease Develop-mental Plagiocephaly in Young Infants. Health. 2014;6 (11):1092-1098.
Jorch G.
Prävention des Plötzlichen Kindstodes, Monatsschr Kinderheilkd. 2010;158:564–569.